Usually the first sign is the walk. Someone who used to cover ground easily starts stopping more, taking breaks they did not need before. Their legs go heavy or numb after a few blocks. Age gets the blame. Joints wear down, muscles lose what they had, and slowing down feels reasonable. A lot of people live with spinal stenosis for years before anyone figures out what it is.
Spinal stenosis symptoms are among the most commonly misattributed complaints in adults over 60. Spinal stenosis builds over years, and what it produces is close enough to normal aging that patients and sometimes their doctors move on without looking deeper.
What Are Spinal Stenosis Symptoms?
Spinal stenosis is a narrowing of the spinal canal that puts pressure on the nerves running through it. That pressure produces pain, numbness, tingling, and weakness. In lumbar stenosis, symptoms appear in the legs and lower back. In cervical stenosis, they appear in the arms, hands, or neck.
Lumbar stenosis is far more common. Spinal stenosis develops gradually over years, which is part of why the early warning signs go unrecognized for so long.
How the Canal Narrows and Why It Hurts
Narrowing does not happen overnight. Bone spurs form on the vertebrae, ligaments thicken, and discs lose height and sometimes bulge inward. Each of these changes is part of normal spinal aging. The problem is when they accumulate together. Once the available space for nerves shrinks past a certain point, the nerves start sending signals that were not there before.
Because the changes build slowly, spinal stenosis symptoms often start as occasional discomfort. A bad day here and there that becomes more frequent over months. By the time the pattern is noticeable, some people have been tolerating the discomfort long enough that it has started to feel like just the way things are.
Spinal Stenosis Symptoms That Mimic Normal Aging
Lumbar spinal stenosis has a characteristic symptom that sets it apart from general back pain: legs that ache or go heavy during walking and ease when sitting down or bending forward. A person might make it two blocks before needing to stop, feel fine on a bench for a few minutes, and repeat the same walk the next day. Over time, walks get shorter without anyone naming a reason.
Clinically this is neurogenic claudication, and forward-flexion relief is its signature. Sitting or leaning over a shopping cart flexes the spine slightly, creating more room in the canal. Standing upright closes that space back down. People with stenosis often instinctively hunch forward when walking and feel better doing so, without knowing why.
Forward lean distinguishes stenosis from vascular claudication, which does not change with position. When back or neck pain becomes an emergency or escalates suddenly, that is a different situation. The more common stenosis pattern is slow-moving and tied to position. It is easy to write off as tired legs.
The Walking Problem That Gets Missed
Spine specialists know the shopping cart sign well, but it rarely reaches patients directly. People notice they feel better leaning on the cart at the grocery store and credit the support. They start choosing routes with more places to sit. Stopping at benches starts to feel normal, and a doctor never hears about it because it seems too minor to mention. Meanwhile the underlying stenosis may be progressing.
Primary care physicians confronted with leg complaints in older patients frequently investigate vascular causes first. Peripheral artery disease produces similar walking symptoms, so a vascular workup is not unreasonable. But if a vascular workup comes back normal and the walking problem persists, the spine deserves attention. Physicians do not always take that step.
Why a Diagnosis Is Often Delayed
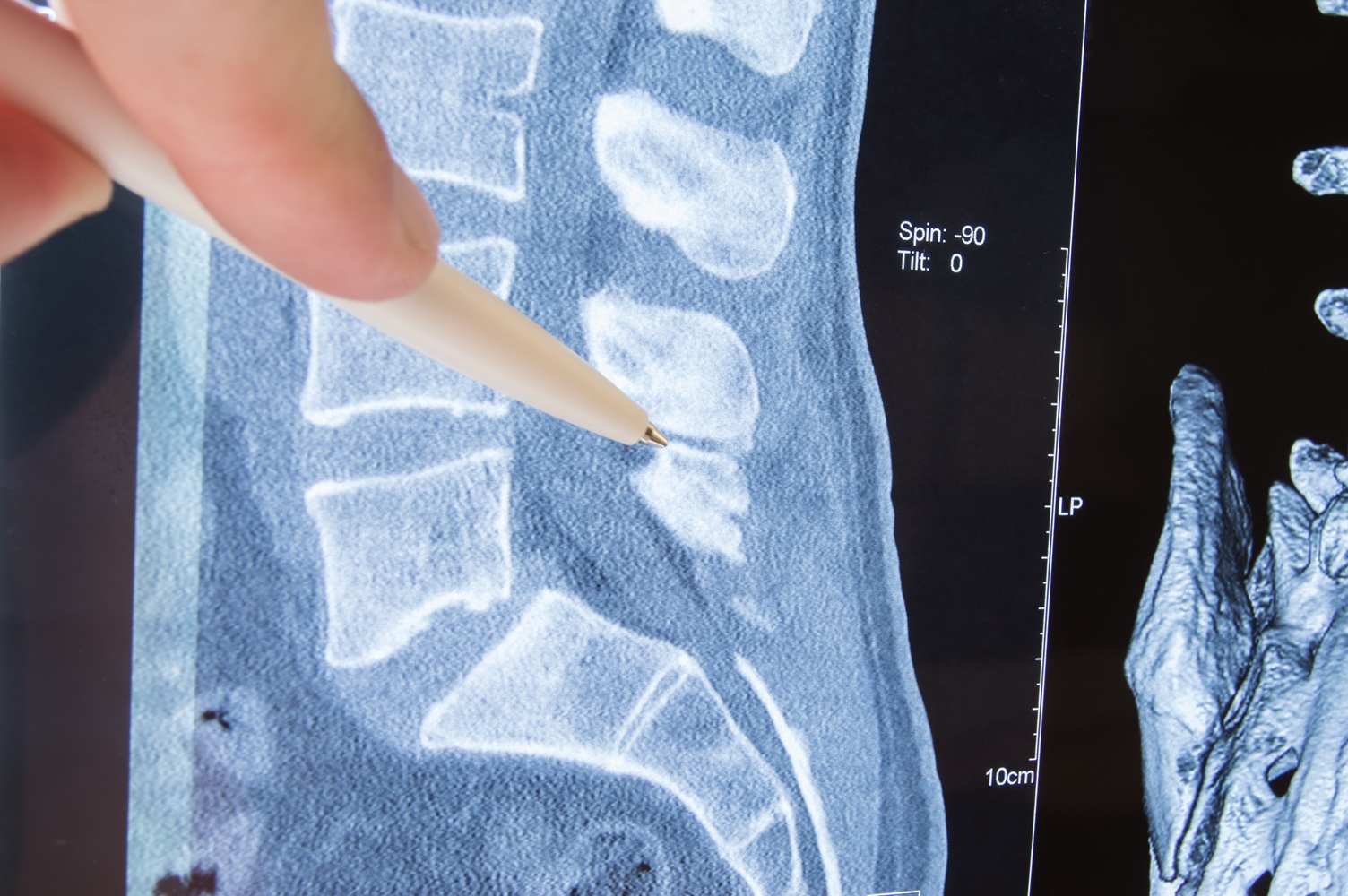
Standard X-rays show bony changes but cannot directly visualize nerve compression. An X-ray of a 65-year-old spine routinely shows disc narrowing, bone spurs, and arthritic changes. A radiologist may note degenerative changes consistent with age, which is accurate, and a primary care physician may relay this as normal aging. Both are technically correct. What neither statement rules out is stenosis. Ruling that out requires a different test.
An MRI shows whether the spinal canal has narrowed enough to compress nerves. Without one, significant stenosis can sit behind a normal-sounding radiology report for years. Patients who eventually receive a stenosis diagnosis often recall a physician telling them their back looked fine on X-ray at some earlier point. No one connected the imaging to the symptom because no one ordered the right test. Stenosis frequently coexists with other spinal conditions, which makes the symptom pattern harder to sort out when a patient describes diffuse back and leg problems.
When Spinal Stenosis Symptoms Require Urgent Attention
Some changes in spinal stenosis symptoms move the situation from watchful waiting to urgent evaluation. Bowel or bladder dysfunction alongside back and leg symptoms suggests cauda equina involvement, which is a surgical emergency. Rapidly progressing leg weakness warrants prompt evaluation. This means weakness that gets meaningfully worse over days or weeks, not the gradual kind building over months. Bilateral leg symptoms, both legs affected at once, typically indicate more significant canal narrowing than one-sided symptoms alone.
When symptoms no longer respond to physical therapy, medication, or steroid injections, minimally invasive surgery is worth discussing with a spine specialist. Endoscopic decompression lets surgeons remove the tissue compressing the nerve through small incisions, with recovery times shorter than traditional open surgery.
What Treatment for Spinal Stenosis Looks Like
People diagnosed with spinal stenosis do not need surgery, at least not at first. Physical therapy focused on flexion-based exercises is usually the starting point. Those exercises train the spine toward positions that open the canal slightly and reduce nerve pressure. Anti-inflammatory medications take the edge off flare-ups. Epidural steroid injections go further, targeting the specific nerve being compressed, and the relief can hold for several months.
Conservative care aims to preserve function rather than reverse the structural narrowing, which degenerative stenosis does not do on its own. What the treatment achieves is a reduction in the inflammation and muscle tension that amplify what the structural problem produces. For a lot of patients, that is enough to stay active for months or years without surgery becoming necessary.
When Surgery Becomes the Next Step
Surgery is typically discussed when conservative care has failed, when daily function has declined significantly, or when the neurological signs above appear. Lumbar laminectomy is the standard procedure. It removes the portion of the vertebra pressing on the nerve. The American Academy of Orthopedic Surgeons reports that laminectomy reliably improves walking ability and leg pain for patients with symptomatic stenosis who have not responded to conservative care.
Functional limitation drives the decision more than pain level. A patient with significant pain who can still walk a reasonable distance and has no neurological symptoms may stay on conservative treatment. A patient with milder pain who can no longer walk half a block is a surgical candidate regardless of how they describe the discomfort.
Questions Worth Asking Your Doctor
Can spinal stenosis get better on its own?
Structural narrowing does not reverse without intervention. Symptoms can fluctuate, and some patients have long stretches where stenosis is less bothersome, but the underlying canal narrowing does not improve over time. Conservative treatment keeps symptoms manageable. It does not address what caused them.
At what age does spinal stenosis usually appear?
Degenerative stenosis is most common after age 50, with prevalence increasing through the 60s and 70s. A smaller number of cases involve a congenitally narrow spinal canal, which can produce symptoms earlier. Over-60 patients are by far the largest group, which is part of why physicians and patients alike attribute spinal stenosis symptoms to general aging rather than a specific structural problem.
Is it safe to keep walking if you have spinal stenosis?
Walking is generally encouraged and is not making the structural problem worse. Sitting relief is temporary, not a warning sign. The exception is if rapidly worsening weakness or bowel and bladder symptoms develop. In that case, rest and prompt evaluation come first.
Talking to Your Doctor About Spinal Stenosis Symptoms
If walking distances have shortened and sitting reliably helps, bring that specific pattern up with a physician directly, not just as leg pain or fatigue. Ask whether a physician has ordered an MRI. A normal X-ray does not rule out stenosis. Getting the right imaging changes what is possible, even when a doctor has attributed spinal stenosis symptoms to aging for years.
Sources
National Institute of Neurological Disorders and Stroke, Spinal Stenosis
American Academy of Orthopedic Surgeons, Lumbar Spinal Stenosis